MESENTERIC PANNICULITIS – THE MYSTERY OF THE FATTY MESENTERY
Introduction:
Mesenteric panniculitis (MP) represents an idiopathic inflammatory disorder involving the adipose tissue of the bowel mesentery, characterized by a variable degree of inflammation, fat necrosis and fibrosis.
The aim of this presentation is to identify MP characteristic features and pathologies that can mimic MP.
Methods:
We retrospectively reviewed 213 patients diagnosed with increased mesenteric fat density on the basis of CT and MRI findings and categorised them according to the characteristic features and the absence or presence of malignancy.
Results:
Our study reveals that MP has a male predominance of 2:1 and affects adults during the sixth and seventh decade of life, which correspond with bibliographic data (1).
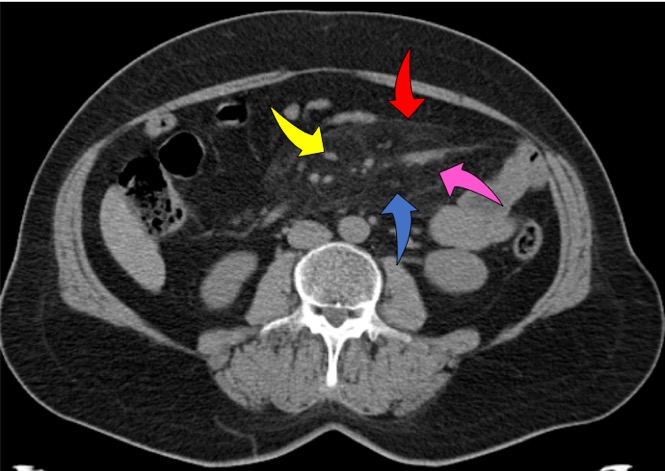
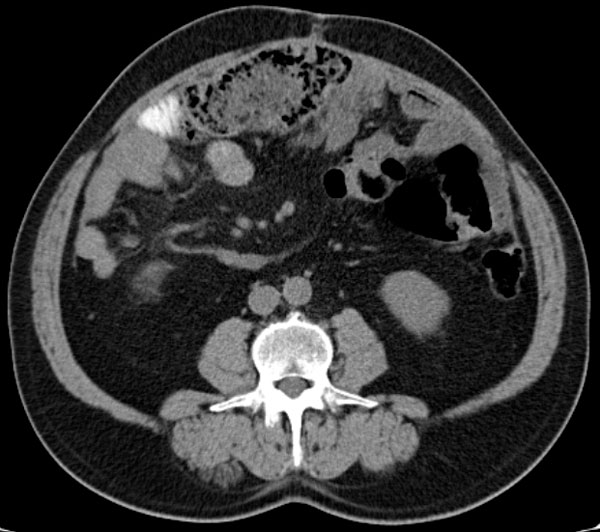
The following imaging signs are responsible for MP:
– increased mesenteric fat density – 100% (pink arrow);
– lymph nodes in the mesentery – 85,91% (yellow arrow);
– „fat halo sign” – 59,62% (blue arrow);
– pseudocapsule – 23% (red arrow).
The exact etiology of MP has not yet been determined. Many factors support the hypothesis that MP is an autoimmune disease. In our study we observed that this disorder can be associated with inflammation (29,57%), intra-/extra-abdominal malignant diseases (18,3%), abdominal surgery or trauma (2,81%), mesentery ischemia (1,4%). In most of cases (47,88%) there were no associated pathologies detected.
Discussions:
The indispensable imaging sign of MP is increased mesenteric fat density, but before suggesting a diagnosis of MP we must exclude alternative causes of the increased mesenteric fat density. MP can also be associated with mesentery ischemia, therefore it‘s important to use i.v. contrast (fig. 3 thrombosis of the superior mesenteric artery green arrow).

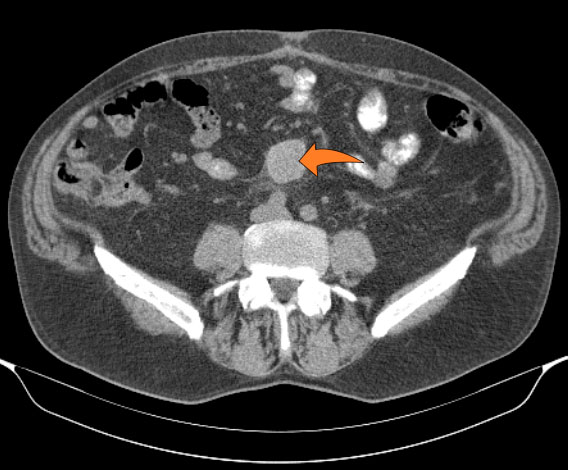
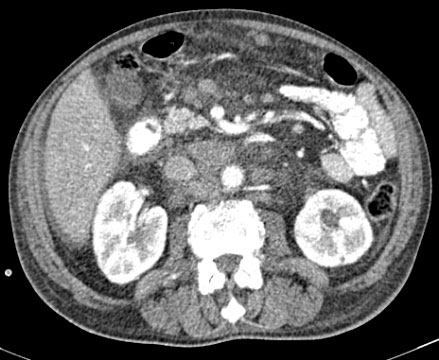
Many malignant processes can mimic MP. The most importan tfeatures that may indicate malignancy are the specific lymph node characteristics like size (>12mm) and the absence of the „fat halo sign“ (orange arrow fig. 4, fig. 5b, fig. 6a & 6b), but the presence of non-specific lymph nodes can not exclude the malignancy (fig. 4).



Conclusions:
1. In most patients, radiologic features of MP included increased mesenteric fat density, lymph nodes in the mesentery and „fat halo” sign.
2. CT appearances vary depending on the predominant tissue component (fat, inflammation, or fibrosis).
3. All patients with CT and MRI features of MP should be evaluated in detail, as some of these features may indicate an associated malignancy.
4. Lymph node size (>12 mm) and the absence of the fat ring sign were identified as predictors of subsequent diagnosis of malignancy in patients with MP.
5. There is one mystery that remains still unknown: Is MP result of different disorders or occurs independently?
References:
1. G. A.Averanga Ticona, Z. Figueroa Marquez , C. Puentes, G. G. Leal, Y. P. Narváez Rojas, J. Crosta, F. A. Abramzon. Mesenteric panniculitis. ¨The fat must also be looked at¨. ECR 2019
2. Grainger & Allison’s Diagnostic Radiology, 6th Edition, 2015; 710-712
3. Filippone, A., Cianci, R., Di Fabio F., Storto ML. Misty mesentery: a pictorial review of multidetectorrow CT findings. Radios Med2011; 351-365